The sequencing engine
A claim walks in.
A cited number
walks out.
Not a rules engine — rules are why the system is stuck. The Claims Genomics Model is a learning system: it turns every claim into a 48-feature genome, learns what normal looks like from your own data, and argues both sides before a human signs.
Step 01 — Sequence
Every claim becomes a genome.
48 features.
Two strands.
One vector.
The care strand carries the clinical truth — diagnoses, trajectory, dose plausibility. The claims strand carries the financial truth — codes, charges, payer behavior. Most systems read one. The genome reads both, together.
An autoencoder learns normal from tens of millions of your own claims — then flags what doesn't reconstruct. No hand-written rules. 28 novel patterns※unsupervised discovery · integrated-payer engagement found this way that no rulebook contained.
Step 02 — Argue
Both sides, against ourselves, on every claim.
A claim's path across the desk.
The same handoff a denied claim walks in a real revenue-cycle shop — each stage has one owner, and payer intelligence feeds the routing the whole way.
surfaced
The genome flags it
The sensor finds the claim and its dollars.
coded
The Coder
Chart vs. billed line — dose & units plausibility.
adjudicated
The Adjudicator
Adjudicable? Cleanest legal posture; timely-filing.

routed
The Router + desk
Right CPAC, signatory & address; desk tailors posture.
audited
The Auditor
No claim without a quote. CLEARED / FIX / HELD.

decided
The Director
One payer-tailored plan; recommends go / no-go.
approved
You
A person clicks Approve & file. Nothing auto-mails.
adversarial by design — CCPRA argues the provider · CCPVA argues the payer · a human rules
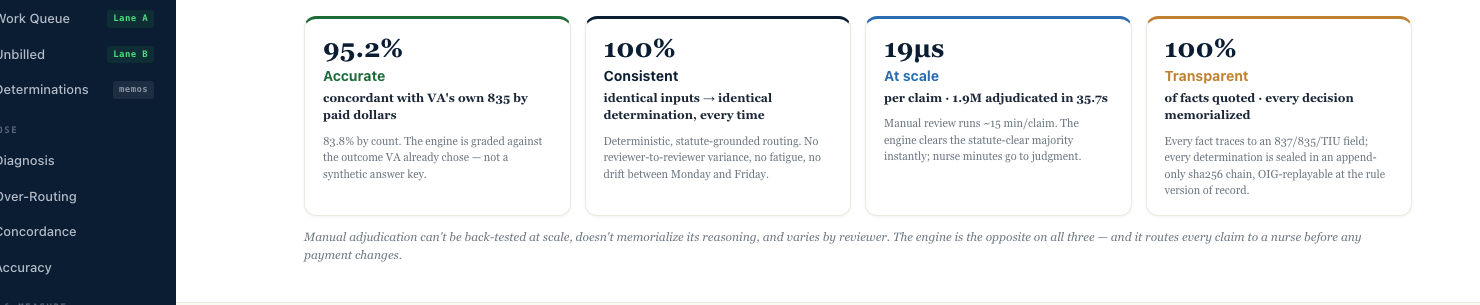
Step 03 — Show the work
Glass-box, or it doesn't ship.
Every determination shows its receipts.
A risk score is an opinion. A determination is a case — cited to the contract clause, the code, the regulation in force on the date of service, and the chart. Defensible to provider, payer, and regulator alike.
The self-review gate blocks ~14% of our own work before it ships. Trust is built by what you refuse to send.
Seven pillars — each cited, each independent
- Contract — rate sheet §4.2, in force on DOScited
- Code — CPT 99291 + MUE limitcited
- Regulation — 38 CFR §17.1002 (layperson std.)cited
- Chart — TIU note within ±3 days of DOSquoted
- Payer policy — versioned by date of serviceon file
- Human authority — reviewer signs the determinationsigned
Step 04 — Move first
Pre-payment, not pay-and-chase.
19 microseconds.
Before the dollar moves.
Recovery is the apology; prevention is the product. The same genome that wins appeals scores every claim pre-payment — so gaming stops paying and pay-and-chase ends.

Step 05 — Hunt where the waste lives
High-volume, low-value — that's where a genomic profile pays.
Everyone audits the whales.
The waste is in the krill.
Inpatient is high-dollar and well-policed — ~2% improper※CMS CERT FY2024. The waste concentrates in millions of small claims a day — where rules engines can't tell a justified course of care from a non-tapering episode. Clinical signal and billing signal have to be read together.
improper-payment rate by service family · sources※CMS CERT FY2024 · OIG A-05-14-00041 · A-09-21-03006 · A-06-23-01002
Medicare FFS average 7.66% · *sampled enrollee-months with any improper line
The provider sees it before the claim goes out — not after a recoupment letter. The patient gets the right service at the right intensity. Abrasion goes down, not up.
Federal-grade, by construction
Built where the bar is highest.
Authorized against the most demanding security baseline in U.S. healthcare, running against VistA, Cerner, and Epic in production. First deployment to a national ATO in under 18 months※VA authorization record.
See it on your data
Bring your 837s and 835s.
We'll show you the DNA.
A scoped read of your claims — the recoverable pool by path, every number with its provenance, in weeks not quarters.